
November 2025




How to read this report
This report contains information on the care delivered by NHS vascular units for:
- people with peripheral arterial disease (PAD) who undergo either (a) lower limb angioplasty / stent, or (b) lower limb bypass surgery, or (c) major lower limb amputation
- people who have a repair procedure for abdominal aortic aneurysm (AAA) or aortic dissection
- people who undergo carotid endarterectomy or carotid stenting.
While various outcomes are included in this report, we focus on short-term postoperative mortality rates across the various procedures because this indicator reflects the safety of the surgery and the quality of perioperative care in preventing life-threatening complications.
Results are typically presented as totals and/or percentages, medians and interquartile ranges (IQR). In a few instances, the percentages do not add up exactly to 100%, which is due to the rounding up or down of the individual values. Unless otherwise stated, results are presented for all four UK nations.
For clarity of presentation, the terms NHS trusts and (vascular) units have been used to describe both NHS trusts and Local Health Boards. A list of NHS vascular units for which results are published is available on the VSQIP website, together with more details of the audit methods. An online glossary is available to explain some of the more technical or medical terms used in this report.
Supplementary materials for this report are available at: www.vsqip.org.uk. These include a description of the audit methods, data tables and an interactive dashboard containing individual NHS trust/health board results on the key NVR metrics, as well as the results for each UK country. The website also provides access to:
- infographics for each of the main procedure types
- links to resources that support local services’ quality improvement initiatives
- links to other sources of information about vascular conditions.
Introduction
The National Vascular Registry evaluates the quality and outcomes of care for adults who had major vascular procedures in NHS hospitals. Its overarching aim is to support vascular services provide high quality of care for these people, and share examples of good practice as well as highlighting areas which merit further investigation in order to improve care. This 2025 State of the Nation report contains key findings for emergency (non-elective) and elective vascular procedures carried out during 2024, along with some outcome indicators for the procedures performed between January 2022 and December 2024 National guidelines underpin the management of people with vascular conditions, and the NVR evaluates patterns of care against these recommendations. An overall framework for vascular services is described by the “Provision of Services for People with Vascular Disease” published by the Vascular Society of Great Britain & Ireland. Additional standards originate from documents published by the National Institute for Health and Care Excellence (NICE), European Society of Vascular Surgery guidelines, national screening guidance, and government documents. From these, and in consultation with its professional and patient advisory groups, the NVR developed five quality improvement (QI) goals and associated indicators, which are published in the NVR Quality Improvement (QI) Plan.
Recommendations
| NVR Key Recommendations | Audience | Results in 2024 | National guidance/standard |
|---|---|---|---|
| 1) Evaluate strategies for reducing long delays to revascularisation for people with chronic limb threatening ischaemia (CLTI), to address lack of improvement in meeting timelines recommended in VSGBI Quality Improvement Framework (QIF) for peripheral arterial disease. (Extended from 2024 SotN recommendation) | Integrated Care Boards (ICBs) (working with Trusts), Local Health Boards, Vascular Networks. | Time from admission to procedure: median = 6 days. 49% of patients are revascularised within 5 days (this was 50% in 2023). | NHS England CQUIN benchmark standard: 65% of people with CLTI have revascularisation within 5 days of (non-elective) admission. |
| 2) Ensure measures to remove causes of avoidable delay are prioritised for people requiring elective aortic aneurysm repair and carotid endarterectomy (CEA), given the lack of improvement in the proportion of people whose wait meets recommended standards. (Extended from 2024 SotN recommendation) | ICBs (working with Trusts), Local Health Boards, Vascular networks, national AAA screening programmes. | Median time for AAA repair: 81 days; 33% of patients were treated within 8 weeks (this was 31% in 2023). Median time for CEA: 14 days; 53% of patients treated within 14 days (this was 49% in 2023). | AAA screening programme standard no. 14: elective AAA repair is within 8 weeks) European Society for Vascular Surgery (ESVS) advise CEA is within 14 days of symptoms. |
| 3) Examine coordination of vascular and supporting services so that people have timely access to major lower limb amputation, ideally being performed on a planned operating list within 48 hours of the decision to operate. | ICBs (working with Trusts), Local Health Boards, Vascular Networks. | The median time from vascular assessment to major lower limb amputation was 9 days (IQR: 3 to 28 days) | VSGBI Amputation Quality Improvement Framework |
| 4) Ensure there is coordinated MDT approach which enables seamless management of people with diabetes who require vascular interventions across primary and secondary care, as they require more intensive management strategies. | ICBs (working with Trusts), Local Health Boards, Vascular networks. Diabetes clinical networks. | The prevalence of diabetes has increased in people having lower limb procedures, being 50.6% among people who had revascularisation, and 62.7% for major amputation. | NICE guideline NG19 (diabetic foot problems) recommendation 1.2: Care-across-all-settings |
| 5) Accelerate review of network pathways and working arrangements across vascular surgery, interventional radiology and anaesthesia to ensure endovascular repair of ruptured aortic aneurysms is available for suitable patients. (Extended from 2024 SotN recommendation). | NHS England Specialist commissioning, ICBs (working with Trusts), Local Health Boards, Vascular networks. | Proportion of repairs of ruptured AAA performed as endovascular repairs was 46% in 2024 (up from 30% in 2018). | NICE guideline NG156 recommendation 1.6: Repairing ruptured aneurysms. The Provision of Services for Patients with Vascular Disease. November 2024. |
1. Lower limb revascularisation procedures
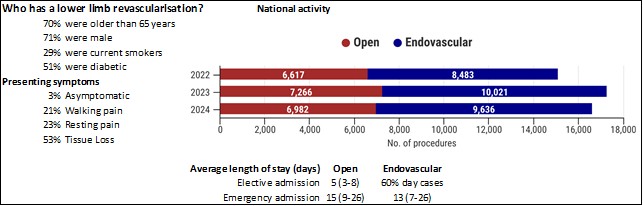
Peripheral arterial disease (PAD) of the lower limbs causes a range of symptoms including pain whilst walking or at rest, ulceration and gangrene, and can lead to loss of a limb. Revascularisation procedures improve blood flow in the legs to alleviate these symptoms, and they can be performed using open surgery, endovascular techniques or a Combined Open with Endovascular Revascularisation procedure (COWER, also known as a hybrid procedure). NHS organisations submitted data on 16,618 lower limb revascularisation procedures performed during 2024 (Figure 1), including:
- 6,982 bypass or open procedures recorded (4,089 elective and 2,893 non-elective). Of these, 2,453 were hybrid revascularisations.
- 9,636 endovascular procedures (6,015 elective and 3,621 non-elective).
The number of hybrid procedures has increased in the recent years and accounted for 14.8% of all lower limb revascularisations in the UK, up from 9.9% in 2020. Estimated case ascertainment rates in 2024 were 89% for bypass (for England = 91%; for Wales = >100%; for Scotland = 42%; for NI = 100%) and 58% for angioplasty (for England = 61%; for Wales = >100%; for Scotland = 6%; for NI = 65%).
The characteristics of patients who had a revascularisation are summarised in Figure 1 (see supplementary material for more details). The prevalence of diabetes has increased from 46.9% in 2020 to 50.6% in 2024. Patients with diabetes and PAD require management from multiple specialists, and the high prevalence highlights the need for integrated vascular-diabetes care pathways.
Figure 1: Summary statistics about people who had a lower limb revascularisation procedure
Time from non-elective admission to revascularisation for people with chronic limb threatening ischaemia (CLTI)
Key messages:
People with CLTI admitted as an emergency are recommended to have revascularisation within 5 days of their admission. In 2024, the proportion revascularised within 5 days was 49%. Among the 60 NHS vascular units performing at least 10 procedures for people with CLTI admitted non-electively:
- 27 units had at least 50% of their patients wait more than 5 days
- 18 units had at least 25% of their patients wait more than 10 days.
Chronic limb-threatening ischaemia (CLTI) is the severest form of PAD, with people often having either rest pain or tissue loss. Timely revascularisation is important for people admitted as an emergency with CLTI because delays increase the risk of limb loss. Among 11,190 people who had revascularisation for CLTI in 2024, there were 5,182 admitted as an emergency (non-elective admission). The median time (IQR) from admission to revascularisation was 6 (3-9) days among these 5,182 individuals. The proportion of people revascularised within 5 days in 2024 was lower than in 2021 (54%).
Outcomes after lower limb revascularisation for PAD
Key messages:
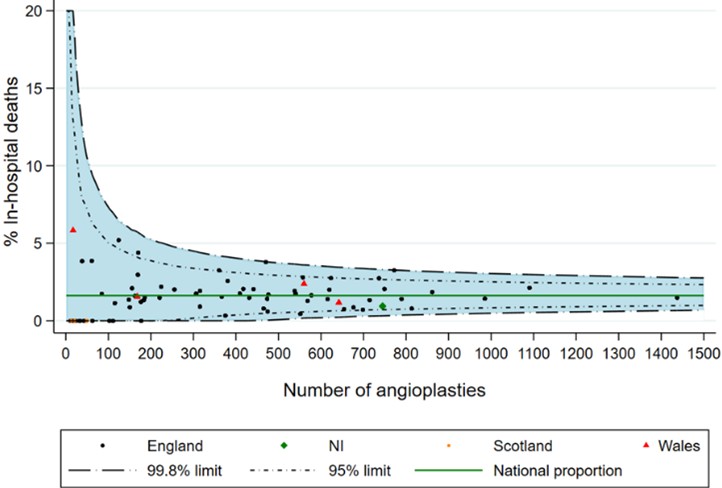
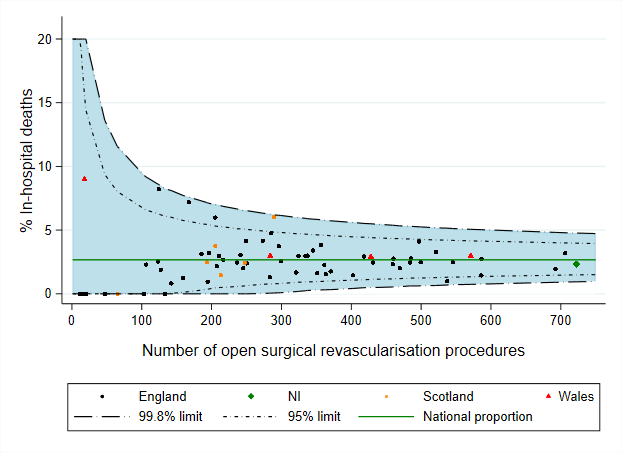
In 2024, the in-hospital postoperative mortality rates for lower limb bypass / open procedures were 1.1% for elective admissions and 4.2% for non-elective admissions. For lower limb angioplasty / stents, rates were 0.7% for elective admissions and 3.6% for non-elective admissions.
In the NHS vascular units that performed bypass / open procedures, the adjusted postoperative in-hospital mortality rates fell within the expected range given the volume of cases performed (national average = 2.7% for 3 years from 2022 to 2024).
In the units that performed lower limb angioplasty / stents, the adjusted mortality rates were within the expected range (national average = 1.6% for 3 years from 2022 to 2024).
For bypass / open procedures, over 85% of patients had no reported complications, and rates of readmission within 30-days were 11.4% for elective and 14.8% for non-elective admissions. For lower limb angioplasty / stents, rates of readmission within 30 days were 10.6% for elective and 19.7% for non-elective admissions.
| Figure 2: Variation in the time from admission and revascularisation for people admitted non-electively with CLTI in 2024 among NHS organisations. The black dots are the median number of days, while the green line shows the interquartile ranges. The red line is the PAD QIF target of 5 days. Graph limited to NHS organisations with a volume of ≥10 non-elective CLTI cases. 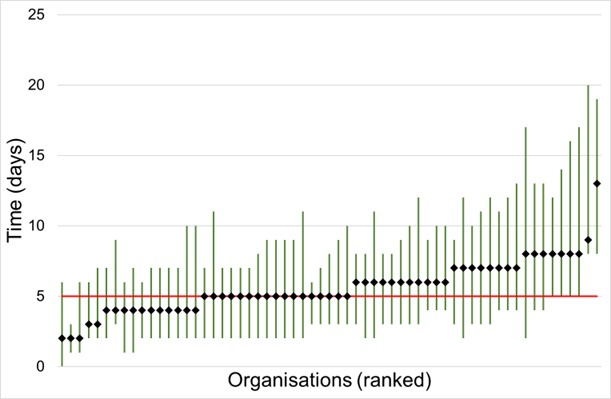 |
Figure 3: Risk-adjusted in-hospital deaths after lower limb revascularisation for NHS organisations from January 2022 to December 2024.
2. Major lower limb amputation
PAD may become sufficiently severe for people to require an amputation of a leg, either above or below the knee. People with diabetes even without PAD may require an amputation due to tissue damage, with or without infection. This section focuses on major (above the level of the ankle) unilateral (one leg only) lower limb amputations. The NVR received details of 3,877 major lower limb amputations performed in 2024, giving a case ascertainment rate of 84% (for England = 87%; for Wales = >100%; for Scotland = 40%; for NI = 100%).
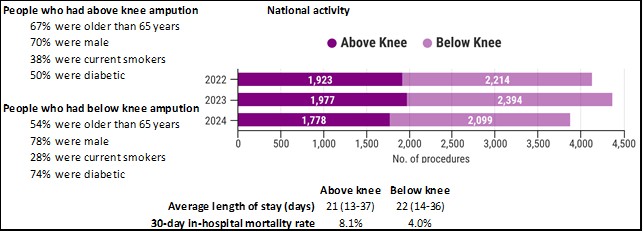
Figure 4 provides an overview of the people who had a unilateral major amputation. In 2024, there were 1,778 above knee (AKA) and 2,099 below knee amputations (BKA), giving an overall AKA:BKA ratio of 0.85. Vascular units should aim to have an AKA to BKA ratio below one, and the majority of NHS vascular units had ratios within the expected range (see supplementary materials).
There were fewer procedures in 2024 compared with 2023, and the increasing trend seen in previous years was no longer evident. The prevalence of diabetes has increased from 56.4% in 2020 to 62.7% in 2024. As noted before, the high prevalence highlights the need for integrated vascular-diabetes care pathways (see supplementary material for more details). Among the AKA procedures, 221 (12.1%) were performed within 30 days of a lower limb revascularisation; for BKA procedures, the figure was 324 (15.1%).
Figure 4: Summary statistics about people who had a unilateral major lower limb amputation
Process measures for people undergoing a major lower limb amputation
Key messages:
All people undergoing major lower limb amputation should be treated in a timely fashion. The overall median time from vascular assessment to major lower limb amputation was 9 days (IQR: 3 to 28 days). Among people admitted non-electively, there were 13 NHS organisations where a quarter of people waited longer than 30 days from vascular assessment to amputation.
It is recommended that major amputations should be undertaken on a planned operating list during normal working hours, and a consultant surgeon should operate or at least be present in the theatre to supervise. In 2024, over 90% of major amputations (BKAs and AKAs) were performed during the day (8am to 6pm), and a consultant surgeon was reported as present for three-quarters of the procedures. In the 55 NHS vascular units with at least 10 procedures in 2024, 34 units reported a consultant was present in theatre for over 80% of procedures.
Figure 5: Variation in the time from vascular assessment to major amputation in 2024 among NHS organisations. The black dots are the median number of days, while the green line shows the interquartile ranges. The red line is 7 days.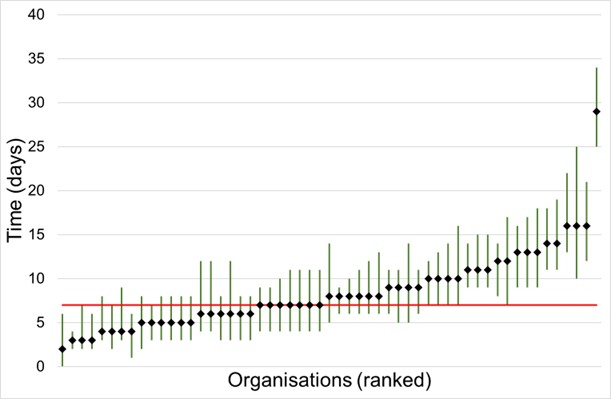 |
Outcomes after major unilateral lower limb amputation
Key messages:
The overall rate of 30-day in-hospital death for major lower limb amputations in 2024 was 5.9%. As expected, it was higher for AKA (8.1%) than BKA (4.0%).
All NHS organisations had an adjusted 30-day in-hospital mortality rate that fell within the expected range of the overall 30-day in hospital mortality rate (national average = 5.9% for 3 years from 2022 to 2024).
Rates of readmission within 30 days were 10.4% for AKAs and 11.6% for BKAs.
Figure 6: Risk-adjusted 30-day in-hospital death rate following major amputation for procedures between January 2022 and December 2024. Overall 30-day in-hospital mortality rate was 5.9%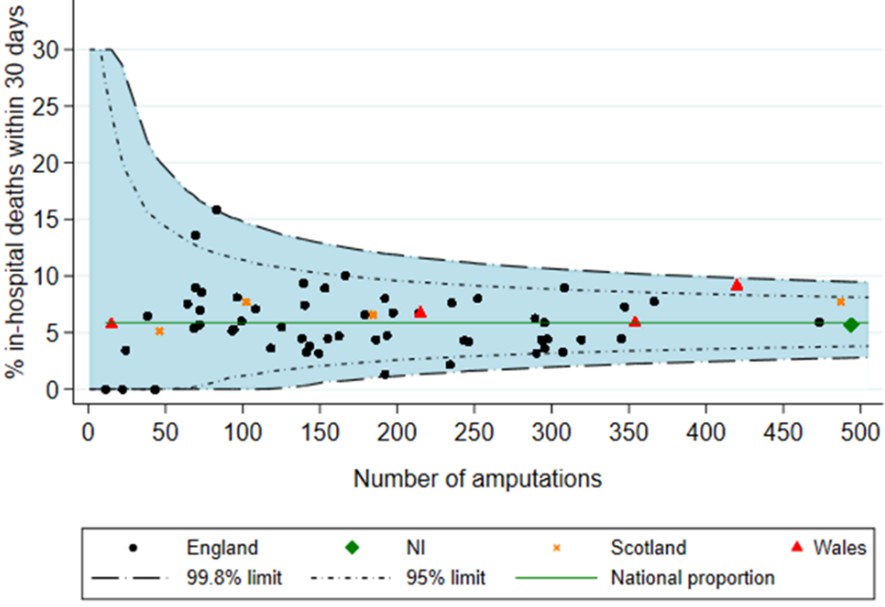 |
4. Aortic Procedures
INTACT INFRA-RENAL ABDOMINAL AORTIC ANEURYSMS (AAA)
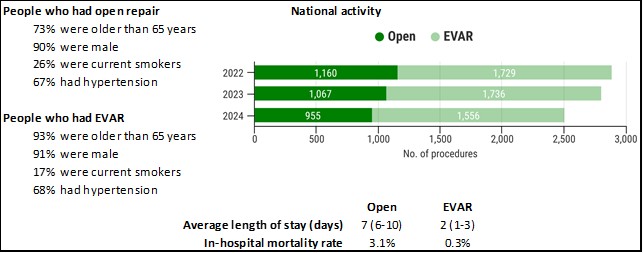
When aneurysms develop in the aorta, they most frequently occur below the arteries to the kidneys, and are known as infra-renal AAAs. The NVR received information on 2,511 people who had an elective repair of an unruptured infra-renal AAA in 2024, which corresponds to an estimated case-ascertainment rate for the UK of 91% (for England = 91%; for Wales = >100%; for Scotland = 64%; for NI = 100%). Of these, 62.0% of procedures were endovascular repair (EVAR) and 38.0% were open repair (Figure 7). This split between EVAR and open repair varied across NHS organisations – among the 59 NHS vascular units that performed elective AAA repair in 2024, 10 units performed EVAR in over 80% of procedures, while 7 units performed EVAR in less than 40% of cases. For more details of patient characteristics, see supplementary materials.
Figure 7: Summary statistics about people who had elective repair for intact AAA
Time from vascular assessment to elective repair for people with intact AAA
Key messages:
Overall, 33% of patients with AAA had their procedure within 8 weeks (compared with 31% in 2023). At two units, a quarter of people waited more than 220 days for their procedure in 2024 (Figure 8).
The National AAA Screening Programme (NAAASP) has defined a standard of 8 weeks from the date of referral from the NAAASP to the date of repair. The NAAASP recommends that NHS organisations should meet this standard for at least 80% of patients. Meeting this standard remains a challenge for the 59 NHS vascular units performing elective repairs in 2024, and the median time from assessment to procedure was 81 days. Most people who had an elective infrarenal AAA repair in 2024 received care consistent with the standards in the Vascular Society AAA Quality Improvement Framework (see supplementary materials).
| Figure 8: Variation across NHS organisations in the time from assessment to treatment (days) for people who had elective infra-renal AAA repair between January and December 2024. The black dot gives median delay, while the green line shows the interquartile range. The red line shows the NAAASP target of 8 weeks (56 days). 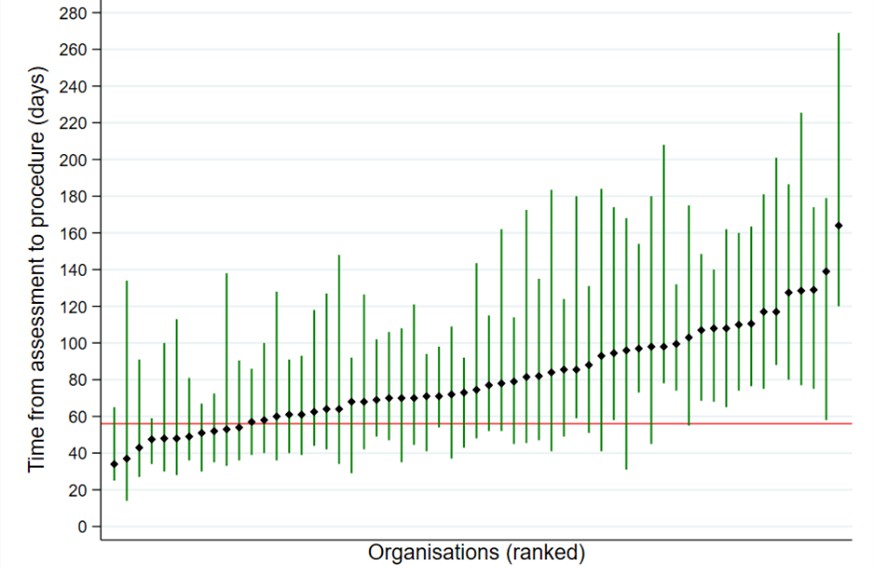 |
Outcomes after elective infra-renal AAA repair
Key messages:
The key outcomes were as follows:
- Mortality was 3.1% for open repair and 0.3% for EVAR.
- Length of Stay was 7 (6 – 10) days for open repair and 2 (1 – 3) days for EVAR.
- Return to theatre was 8.6% for open repair and 2.6% for EVAR.
- Readmission within 30 days was 5.6% for open repair and 5.4% for EVAR.
- For EVAR, the rates of post-op endoleaks were primarily Type 1 (5%) and Type 2 (14%).
Between January 2022 and December 2024, the risk-adjusted in-hospital mortality rates for all NHS vascular units were within the expected range, as defined by the national average of 1.3%.
| Figure 9: Risk-adjusted in-hospital mortality rates after elective infra-renal AAA repair among NHS vascular units (Jan 2022 – Dec 2024). Overall in-hospital mortality rate was 1.3% 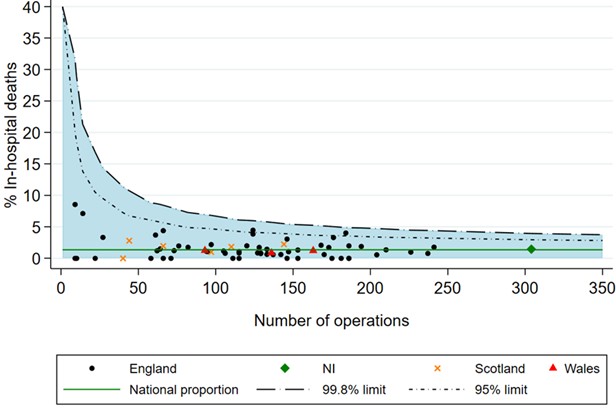 |
REPAIR OF THORACIC AORTIC CONDITIONS
People who suffer from a thoracic aortic aneurysm or aortic dissection are increasingly treated using a thoracic endovascular aortic repair (TEVAR). This procedure is performed in either a cardiothoracic unit or specialist vascular unit. People may present as an emergency admission and have a TEVAR with minimal delay; in some people, the condition may be without symptoms and may be safely treated electively. In 2022-24, there were 432 emergency and 428 elective TEVAR procedures performed by 41 UK vascular units (Figure 10).
Figure 10: Summary statistics about people who had a repair of thoracic aortic conditions
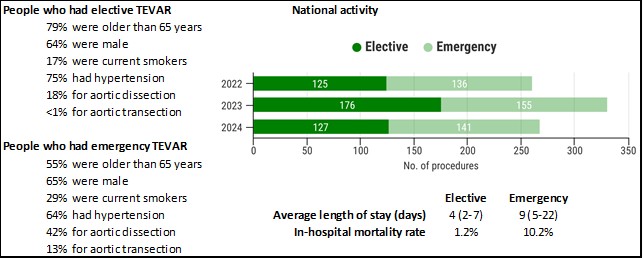
In 2022-24, in-hospital postoperative mortality rates after TEVAR were 10.2% for emergency and 1.2% for elective procedures performed by UK vascular units. Rates of readmission within 30 days were 8.8% for elective procedures and 9.1% for emergency procedures.
REPAIR OF RUPTURED ABDOMINAL AORTIC ANEURYSMS (rAAA)
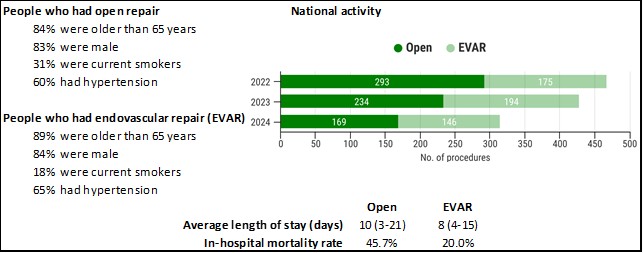
The NVR recorded 1,211 emergency repairs of a ruptured abdominal aneurysm between January 2022 and December 2024, with a fall from year to year (Figure 11). The numbers have decreased significantly since 2015 when over 900 repairs were performed, compared to 315 in 2024. Estimated case ascertainment in 2022-2024 was 94% (for England = 92%; for Wales = >100%; for Scotland = 73%; for NI = 100%).
Key messages:
In 2024, 46% of people with ruptured AAA had an EVAR procedure. Between 2022 and 2024, there was variation across units in the proportion of procedures performed as EVAR, with around a third of units performed more EVARs than open repairs for ruptured AAA. There may be potential in expanding the use of EVAR for ruptured AAA.
For people with rAAA treated in 2022-2024, the in-hospital postoperative mortality rates for EVAR and open repairs were 20.0% and 45.7%, respectively. We caution against comparing these mortality figures for EVAR and open repair because people who have open procedures may represent the more complex cases that are unsuitable for endovascular repair. Rates of readmission within 30 days were 7.4% for open repair and 9.0% for EVAR. During the three-year period 2022-2024, all NHS organisations had in-hospital postoperative mortality rates within the expected range after repair for ruptured AAA. The overall national average mortality rate for this period was 34.8%.
Figure 11: Summary statistics about people who had an emergency repair of ruptured AAA
OTHER ELECTIVE REPAIR OF AORTIC CONDITIONS (COMPLEX ANEURYSMS)
A person can have an aortic aneurysm above or around the arteries to the kidneys. It is common to repair the aorta in these situations using endovascular procedures, although open repairs are indicated when an individual is not suitable for an endovascular approach. The most common procedures are Fenestrated EVAR (FEVAR) and Branched EVAR (BEVAR), which are performed when the aortic aneurysm is close to or involves other arteries branching from the aorta. In 2022-24, there were 1,532 endovascular procedures (which included 1,216 FEVAR and 290 BEVAR procedures) and 253 complex open repair procedures. The majority of the procedures were performed in men (86%). Over 80% were current or ex-smokers.
Key messages:
Postoperative mortality rates were lower after complex endovascular repairs (1.5%) than after complex open repairs (9.9%). Rates of readmission within 30 days were 9.7% for open procedures and 7.3% for endovascular procedures.
URGENT UNRUPTURED AORTIC ANEURYSM PROCEDURES
Some people have their intact AAA repaired after being admitted as an emergency admission (or are recorded as having an emergency operative procedure after an elective admission). Between 2022 and 2024, the NVR received details of 1,418 such cases. These patients tend to have larger aneurysms [6.5 cm (5.6 – 8.0) for any unruptured emergency admission] and have worse outcomes as they tend not to have had the pre-operative work-up, when compared to electively admitted AAA repairs. Postoperative mortality rates were 2.7% for endovascular repairs and 7.0% for open repairs.
REVISION AORTIC PROCEDURES
Since 2020 the NVR has collected information on different types of revision procedures that may be required after an initial primary aortic repair procedure (open and endovascular). These procedures are undertaken to address disease progression or complications from the original procedure, and they represent a growing component of vascular unit activity. Between 2022-2024, the NVR received information about 726 elective revision procedures and 373 non-elective revisions. Common elements of these procedures (more than one element can be undertaken) in each revision included:
- Removal (explant) of a previously inserted graft: 73 elective; 59 non-elective
- Insertion of a new stent graft within / alongside the existing graft (relining): 199 elective; 160 non-elective
- Insertion of a new stent graft to extend the repair into the iliac arteries (distal extension): 243 elective; 94 non-elective
- Embolisation for an endoleak complication after an EVAR procedure: 151 elective; 42 non-elective.
Postoperative mortality rates for elective and non-elective revision AAA procedures were 1.8% and 14.2%, respectively.
5. Carotid endarterectomy
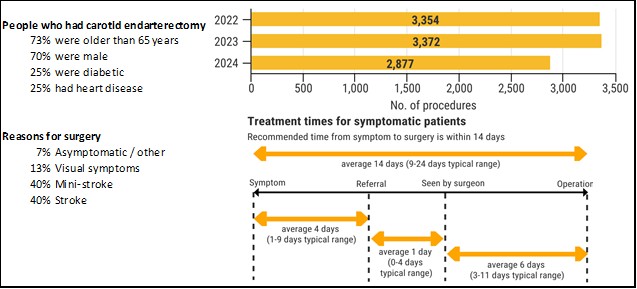
A carotid endarterectomy (CEA) is performed to remove plaque that has built up within the carotid arteries (the main vessels that supply blood to the brain, head and neck), with the aim of reducing the risk of stroke. It is performed in people who have recently experienced symptoms, but it can also be performed in people with no symptoms when the carotid arteries are partially blocked. Symptomatic patients made up around 95% of the CEAs performed in the UK during 2024.
In 2011, there were nearly 6,000 CEAs performed in the NHS. Since then, the number of procedures has fallen substantially (see Figure 12). In 2024, a total of 2,877 CEAs were entered onto the NVR, which corresponds to an estimated case ascertainment for the UK of 87% (for England = 87%; for Wales = >100%; for Scotland = 55%; for NI = 100%). A few vascular units also perform carotid stenting; there are around 50 of these annually.
Figure 12: Summary statistics about people undergoing carotid endarterectomy
Time from symptom to carotid surgery
Key messages:
The time from symptom to carotid surgery is recommended to be within 14 days to reduce the risk of people developing a stroke. The median time from symptom to surgery for people with symptoms who had CEA in 2024 was 14 days and 53% were treated within 14 days. This is slightly better than in 2023 when the median time was 14 days and 49% of people were treated within 14 days. The 14-day-treatment figure was 56% in 2019 (prior to the pandemic). There is still variation in the waiting times for CEA between NHS organisations (Figure 13). The median time exceeded 20 days at eleven NHS organisations. Factors associated with increased delays merit further investigation at a local level.
| Figure 13: Variation across NHS organisations in median times from symptom to procedure for CEA performed between January and December 2024. The black dot gives the median delay, while the green lines show the interquartile range. The red line shows the national target of 14 days. 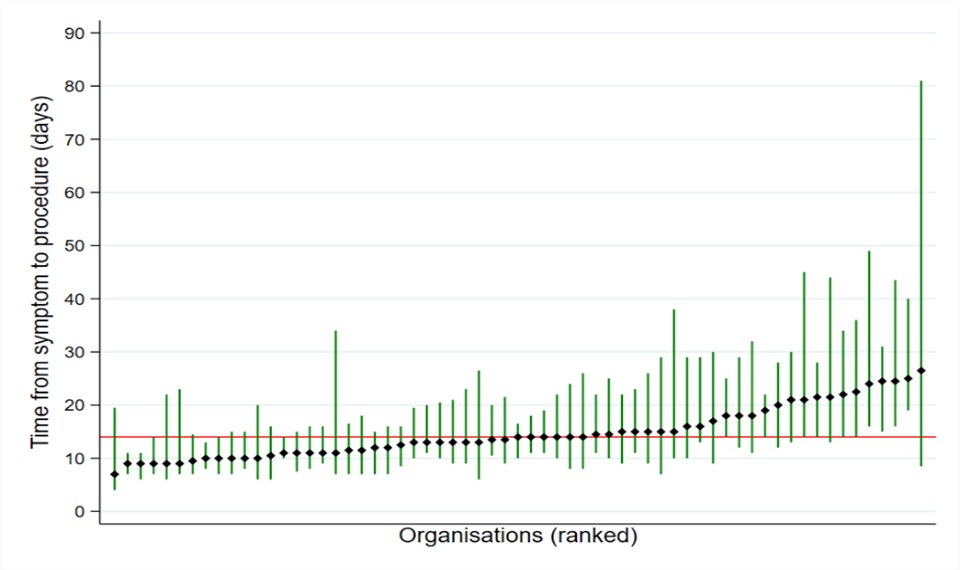 |
Outcomes after carotid endarterectomy
Key messages:
Among the 2,877 people undergoing CEA in 2024, complication rates were:
1.9% of people died and/or had a stroke within 30 days (95% CI 1.4-2.4)
1.4% of people had a cranial nerve injury during their admission (95% CI 1.0-1.9).
Rate of readmission within 30 days was 4.9%. Average length of stay was 2 days (IQR: 1 to 4 days). For CEAs performed between 2022 and 2024, all NHS organisations had an adjusted 30-day mortality / stroke rate after surgery within the expected range of the national average (1.8%) (Figure 14).
| Figure 14: Risk-adjusted rates of stroke / death within 30 days for NHS organisations that performed carotid endarterectomy (2022 to 2024). The national average in these years was 1.8% 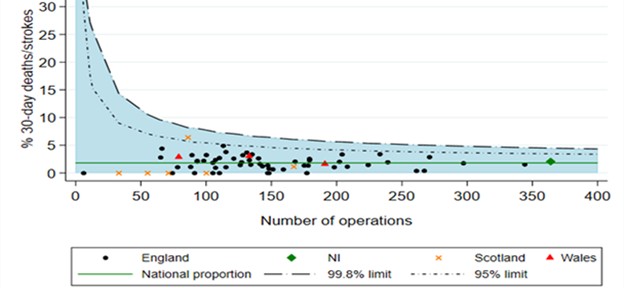 |
6. Commentary
The 2025 NVR State of the Nation report highlights the continuing challenges experienced by NHS vascular services during 2024. The times from vascular assessment and admission to treatment for lower limb revascularisation, AAA and CEA remain longer across the NHS with only a minority of vascular units managing to treat more than half of their patients within target time scales. QI projects to address these delays are a priority, particularly for those organisations with the most significant delays. We encourage units to investigate options for improving referral pathways, capacity, and working arrangements across vascular surgery, interventional radiology and anaesthesia, especially as there has been little or no improvement over the last few years.
More positively, the adverse outcomes reported by vascular units remain low and demonstrate the safe delivery of vascular interventions. The in-hospital mortality rate after open repair of ruptured AAA remains high, and exceeds the rate observed for EVAR. This may be because open repairs are more complex cases that are unsuitable for EVAR. Nonetheless, variation across vascular units in the proportion of EVAR procedures for people with rAAA suggest vascular networks should review access to rEVAR. This requires (i) having hybrid operating theatres available on 24/7 basis, and (ii) developing teams to deliver EVAR for rAAA out of hours, which may include EVAR trained clinicians, nursing staff and radiographers with vascular anaesthetic support.
The mix of vascular procedures continues to change: over the last three years, the number of procedures for infra-renal AAA repair and repair of ruptured AAA have decreased, along with the number of carotid endarterectomies, which may reflect a reduction in the incidence of the indications for these procedures. The reduction in the number of major amputations is encouraging, although the reasons for this are unclear. We note fewer lower limb revascularisations were also entered onto the NVR. The prevalence of diabetes among these patients has increased (particularly for below the knee amputations), and this highlights the need for integrated vascular-diabetes care pathways.
The data entered onto the NVR is generally of high quality, but there are various areas which should be priorities for NHS vascular units and vascular networks to monitor, and remove barriers to the efficient collection of data. We highlight the need to ensure complete entry of endovascular lower limb revascularisation procedures (particularly those performed in day surgery units). Units should also ensure the permission to submit NHS/CHI/H&C numbers is collected from patients, as these identifiers enable NVR records to be linked with external administrative datasets for the evaluation of long-term outcomes. The proportion of NVR records containing the patient’s national identifier was 86% in 2024; compared to 93% in the National Joint Registry.
Finally, the depth of coding within the admitted patient care data from PEDW was lower in 2023/24 and this has meant there were more vascular procedures entered on the NVR than identified within PEDW. This has meant that the case ascertainment figures for health boards in Wales should be interpreted with caution.
This report was prepared by
Clinical Effectiveness Unit, The Royal College of Surgeons of England
Mr Sam Waton, NVR Project Manager
Dr Amundeep Johal, Senior Statistician
Dr Qiuju Li, Research Fellow in Medical Statistics
Dr Frances Sheehan, NVR Clinical Research Fellow
Dr Panagiota Birmpili, NVR Clinical Research Fellow
Prof David Cromwell, CEU Director
Vascular Society of Great Britain and Ireland (VSGBI)
Prof Arun Pherwani, Consultant Vascular Surgeon
Prof Colin Bicknell, Consultant Vascular Surgeon
British Society of Interventional Radiology (BSIR)
Dr Robin Williams, Consultant Interventional Radiologist
Dr James Harding, Consultant Interventional Radiologist
| The Royal College of Surgeons of England is an independent professional body committed to enabling surgeons to achieve and maintain the highest standards of surgical practice and patient care. As part of this, it supports Audit and the evaluation of clinical effectiveness for surgery. Registered charity no: 212808. The RCSEng managed the publication of the 2025 State of the Nation Report. |
| The Vascular Society of Great Britain and Ireland is the specialist society that represents vascular surgeons. It is one of the key partners leading the audit. Registered charity no: 1102769. |
| The British Society of Interventional Radiology is the specialist society that represents interventional radiologists. It is again, one of the key partners leading the audit. Registered charity no: 1084852. |
Commissioned by
 | The National Vascular Registry is commissioned by the Healthcare Quality Improvement Partnership (HQIP) and funded by NHS England and Welsh Government as part of the National Clinical Audit and Patient Outcomes Programme Registered charity no: 1127049. |
Copyright All rights reserved. No part of this publication may be reproduced in any form (including photocopying or storing it in any medium by electronic means and whether or not transiently or incidentally to some other use of this publication) without the written permission of the copyright owner. Applications for the copyright owner’s written permission to reproduce any part of this publication should be addressed to the publisher.
Copyright © Healthcare Quality Improvement Partnership, November 2025
Please cite this report as: Waton S, Johal A, Li Q, Sheehan F, Birmpili P, Cromwell DA, Williams R, Harding J, Pherwani AD, Bicknell CD. National Vascular Registry: 2025 State of the Nation Report. London: The Royal College of Surgeons of England, November 2025.